前言
兩者不管從體驗或精神治癒效果,都能看做類似的啟靈藥。是除了 MDMA 以外有最多精神治療論文的啟靈物質。然而 LSD 體驗時長久於裸蓋菇鹼,實驗成本高,研究落後裸蓋菇鹼幾年。
常見體驗內容(覺知改變、時間扭曲、情緒釋放、自我解構、神祕感、視覺幻象)兩者幾乎都能出現,但 LSD 與裸蓋菇鹼在情緒基調、思維結構、與主題導向有不同的偏重。
可以想像成兩個重疊 70% 的圓,兩著都是作用於大腦 5-HT2A 受體導致的網絡解耦與連結重組,但 LSD 因為多受體作用(含 D2、5-HT1A、adrenergic),會更「清醒、線性、能量高」;裸蓋菇鹼代謝快、峰值集中 , 更「情緒化、有機、象徵性強」。
基礎體驗差異
體驗時長:
藥效與劑量正相關,且 LSD 久於裸蓋菇鹼。
- 裸蓋菇鹼 25 mg 平均主觀效應為 5.5 ± 1.6、30 mg 為 6.4 ± 2.2 小時,通常認為 4-6 小時結束 (Holze et al., 2023)
- LSD 100 µg 平均主觀效應約 8 小時、200 µg 約 11 小時 (Dolder et al., 2017)
起效時間:
- 裸蓋菇鹼:約 30–60 分鐘
- LSD:約 60–90 分鐘
尾段殘效:
- 裸蓋菇鹼:較短,當天可恢復
- LSD:常延續至隔日(較容易導致失眠)
體驗敘事的主題差異
裸蓋菇鹼研究中常見主題:
與萬物合一、重新與家人連結、死亡與重生意象、宗教/靈性接納、強烈與深層的情緒(喜悅、平靜、愛)、超越時空、永恆與感恩感 (Griffiths et al. 2011)
LSD 研究中常見主題:
認知清明、思緒開闊、情緒釋放與關係修復、對死亡與存在議題的洞見、自我界限鬆動、宇宙數學或能量的秩序、創造性洞見與問題解構
(Gasser et al., 2014; Carhart-Harris et al., 2016; Holze et al., 2022)
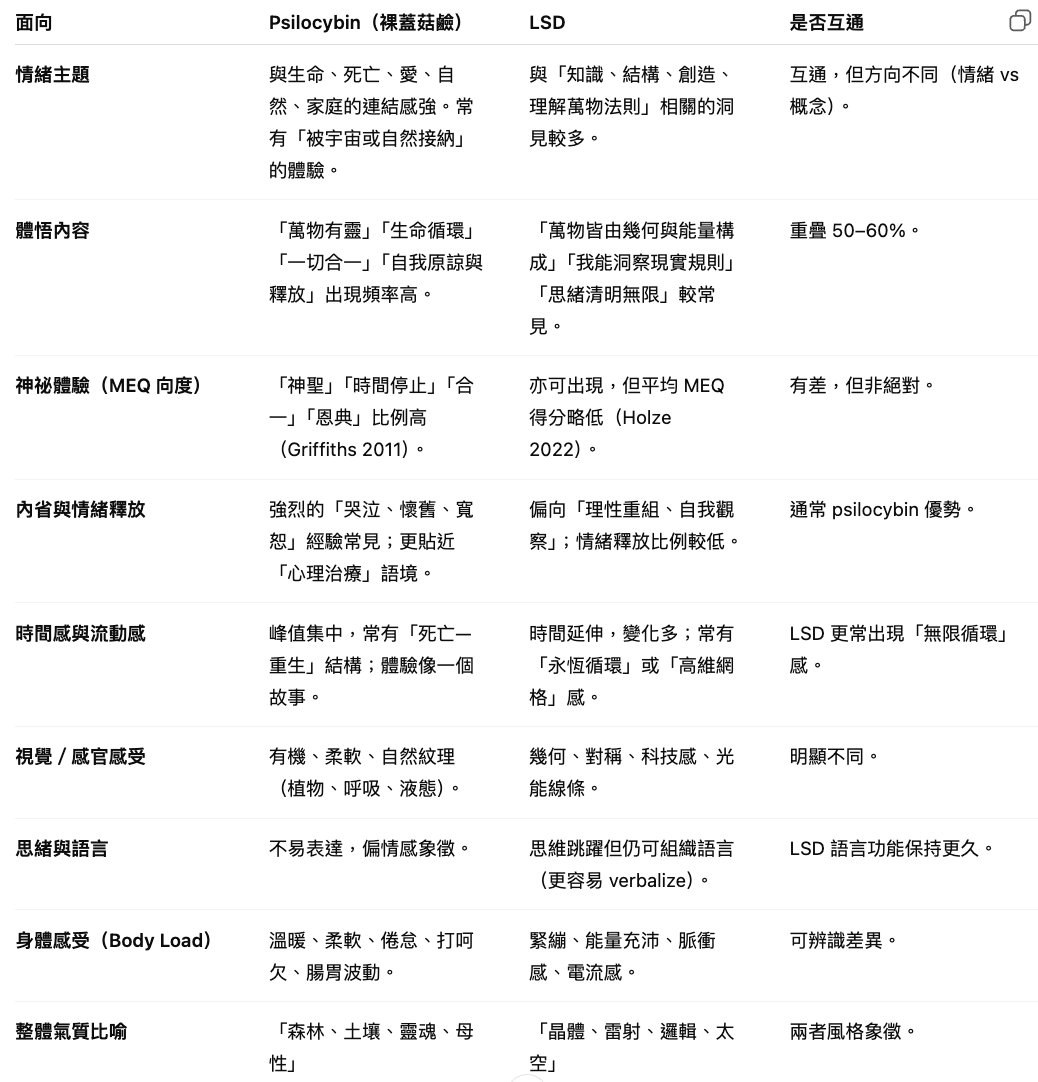
體悟與感受差異
常見體驗出現比例
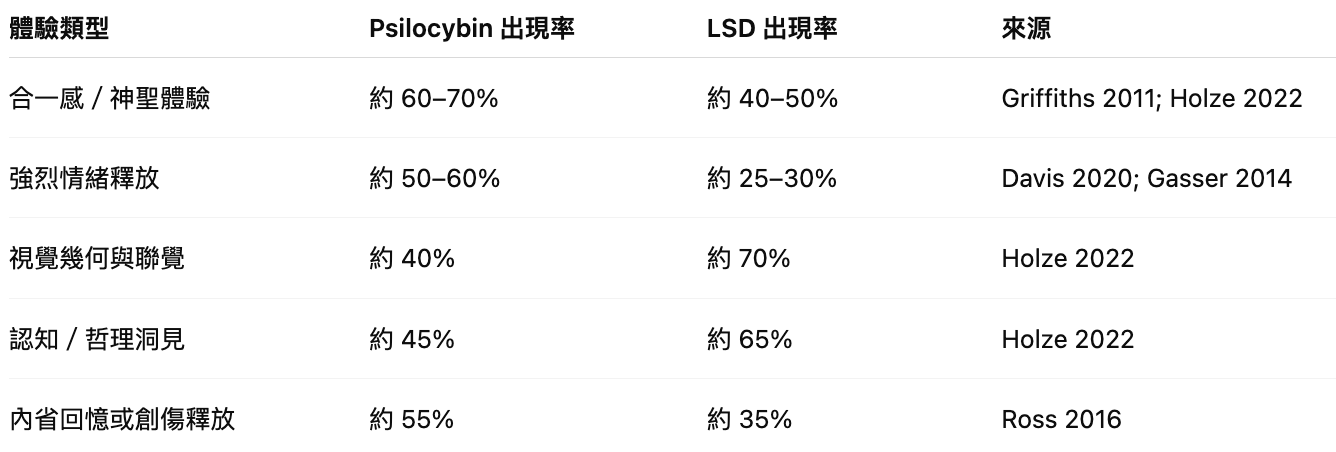
因此裸蓋菇鹼更適合首次使用受試者,當前研究數量也遠多於 LSD。
結論
LSD 與裸蓋菇鹼的體驗沒有絕對界線,它們的差異更像語氣的差異而非語彙的不同。
裸蓋菇鹼偏向心靈與情感性整合,適合自我覺察與溫和探索;LSD 偏向思維與知覺的解析與延展,適合進階者或藝術創造類體驗。一個讓受試者感覺一切都被愛所連結,一個是讓受試者看見一切如何被邏輯所連結。
Holze, F., Becker, A. M., Kolaczynska, K. E., Duthaler, U., & Liechti, M. E. (2023). Pharmacokinetics and pharmacodynamics of oral psilocybin administration in healthy participants. Clinical Pharmacology & Therapeutics, 113(4), 822–831.
Dolder, P. C., Schmid, Y., Steuer, A. E., Kraemer, T., Rentsch, K. M., Hammann, F., & Liechti, M. E. (2017). Pharmacokinetics and pharmacodynamics of lysergic acid diethylamide in healthy subjects. Clinical Pharmacokinetics, 56(10), 1219–1230
Griffiths, R. R., Johnson, M. W., Richards, W. A., McCann, U. D., & Jesse, R. (2011). Psilocybin occasioned mystical-type experiences: Immediate and persisting dose-related effects. Psychopharmacology, 218(4), 649–665.
Gasser, P., Kirchner, K., & Passie, T. (2014). Safety and efficacy of lysergic acid diethylamide-assisted psychotherapy for anxiety associated with life-threatening diseases: A randomized double-blind, active placebo-controlled phase 2 study. Journal of Nervous and Mental Disease, 202(7), 513–520.
Carhart-Harris, R. L., Muthukumaraswamy, S., Roseman, L., et al. (2016). Neural correlates of the LSD experience revealed by multimodal neuroimaging. Proceedings of the National Academy of Sciences USA, 113(17), 4853–4858.
Holze, F., Liechti, M. E., et al. (2022). Direct comparison of the acute effects of LSD and psilocybin in healthy subjects. Neuropsychopharmacology, 47(6), 1215–1226.
Davis, A. K., Barrett, F. S., May, D. G., Cosimano, M. P., Sepeda, N. D., Johnson, M. W., Finan, P. H., & Griffiths, R. R. (2020). Effects of psilocybin-assisted therapy on major depressive disorder: A randomized clinical trial. JAMA Psychiatry, 78(5), 481–489.
Ross, S., Bossis, A., Guss, J., Agin-Liebes, G., Malone, T., Cohen, B., Mennenga, S. E., Belser, A., Kalliontzi, K., Babb, J., Su, Z., Corby, P., & Schmidt, B. L. (2016).
Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depression in patients with life-threatening cancer: A randomized controlled trial. Journal of Psychopharmacology, 30(12), 1165–1180.
Holze, F., Becker, A. M., Kolaczynska, K. E., Duthaler, U., & Liechti, M. E. (2023).
Pharmacokinetics and pharmacodynamics of oral psilocybin administration in healthy participants. Clinical Pharmacology & Therapeutics, 113(4), 822–831.